Last December, Gates of Vienna reported on the hostage taking by the Libyan government of a Palestinian doctor and the Bulgarian nurses. Their imprisonment began in 1999, on trumped-up charges that they were responsible for the spread of HIV to hundreds of children at a pediatric hospital in the city of Benghazi.
But the truth is more cynical and more complicated than Gaddafi’s callous lie about their wrongdoing. From Le Monde here is the succinct version of the whys and wherefores of this travesty:
‘It has been proven and demonstrated that the Bulgarian nurses and the Palestinian doctor are hostages of Gaddafi’, the Moroccan writer and the Gonkur literature award winner Tahar Ben Jelun writes in an article published in the French daily Le Mond.
This is a scandal, that deserves condemnation, just as every other taking of hostages’, he writes.
‘Muammar Gaddafi, who has made the political and moral mistake to admit the responsibility of the country for the attack over Lockerby and against a French town Niger undirectly, by paying the compensations is now trying to do the opposite — to restore the money from a different place and to calm the anger of the families, ruined by the misfortune. Thus we are entering the logic of the Libyan tradition, which can be called ‘blood money’.
‘After I visited Libya in 2004 on invitation by the French Ambassador I found out how far this country is from any democratic state’, Jelun writes.
The reality for these children and their families is a scandal shared by Gaddafi and his grasping paranoid tyranny, the World Health Organization and its sloppy approach to medical care, and the EU, with its refusal to do anything but engage in impotent negotiations. “Negotiate” here means “act like the US State Department”: wring your hands, make empty noises and then claim the credit for having done something when things start to move. Here’s the news release on their hard work:
The Portuguese EU presidency will continue working for the freedom of the five Bulgarian nurses sentenced to death in Libya, just like its German predecessor did.
It will work in close co-operation with the European Commission and Bulgarian authorities so that the nurses return home.
“Close cooperation” so far has translated into eight years in prison for these innocent people. So does that mean eight more years of languishing in jail on the whim of a crazy man determined on revenge for the payout on Lockerbie?
There is no doubt of their innocence — not that it matters. As I reported back in December:
DNA analysis has confirmed that the virus that infected the children could not possibly have been spread by the accused nurses, since it was present before they arrived. But the Libyans aren’t about to let the facts stand in the way of a good infidel hanging.
Gaddafi knows they’re innocent, too. However, he wants his money back from his Lockerbie payout, and he’ll use the suffering of children and their families to get it. That is his whole motive for this caper.
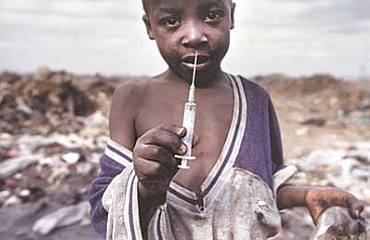
 Meanwhile, the real cause for the infection of these children, and children all over Africa, is reusable needles rather than one-time retractable syringes that prevent needles from being used a number of times thus increasing the risk for the spread of HIV.
Meanwhile, the real cause for the infection of these children, and children all over Africa, is reusable needles rather than one-time retractable syringes that prevent needles from being used a number of times thus increasing the risk for the spread of HIV.
An essay on the situation is here:
An expanding body of evidence challenges the conventional hypothesis that sexual transmission is responsible for more than 90% of adult HIV infections in Africa. Differences in epidemic trajectories across Africa do not correspond to differences in sexual behavior. Studies among African couples find low rates of heterosexual transmission, as in developed countries. Many studies report HIV infections in African adults with no sexual exposure to HIV and in children with HIV-negative mothers. Unexplained high rates of HIV incidence have been observed in African women during antenatal and postpartum periods. Many studies show 20%-40% of HIV infections in African adults associated with injections (though direction of causation is unknown). These and other findings that challenge the conventional hypothesis point to the possibility that HIV transmission through unsafe medical care may be an important factor in Africa’s HIV epidemic. More research is warranted to clarify risks for HIV transmission through health care. [my emphasis]
Meanwhile, the International Council of Nurses has expressed their shock at the lack of adequate nursing care provided by WHO. In May of this year, they issued a press release questioning the practices of the World Health Organization:
– – – – – – – – – –
The governing assembly of the International Council of Nurses (ICN) was shocked to learn of the decline, from an already unacceptably low level, in the number of nurse and midwife posts across all regions and clusters of the World Health Organization (WHO). The data from the WHO human resources report to the 2007 World Health Assembly, revealed that of the health care professionals working on staff at the WHO a mere 1.3 % are nurses; 91.6 per cent are physicians. At 1.8%, dieticians and nutritionists have greater representation than nurses. ICN’s Council of National Representatives (CNR) also learned that the key position of WHO Chief Scientist for Nursing and Midwifery has been reduced to part time due to other assigned roles time and staff support for this office is contracted on short term and part time bases.
This virtual absence of the nursing voice in WHO policy and implementation threatens all WHO programmes, contradicts the organisation’s claim to be addressing the current global crisis in health human resources — focused mostly on nursing, and undermines the effort to attain the Millennium Development Goals (MDGs).
Bill Gates and all the entertainment personalities who have pledged so much money to Africa’s health care could do wonders with one simple move: insist on only retractable, one-use needles for vaccinations. Then children wouldn’t follow hospital garbage trucks to the dump so they can scrabble through bacteria-laden refuse (in their bare feet) to find used needles to sell.
And where is the Live Aid concert to get these nurses out of jail? Or even to get more native nurses trained in Africa? Where’s the push for real health initiatives instead of the agenda-driven WHO philosophy?
How about Gaddafi? He responds to money and to viable threats to his reign, but not much else. Now he wants ten million for each child from that hospital in Benghazi: by some amazing coincidence, the same amount he had to pay for each victim of Lockerbie.
Meanwhile, the nurses and doctor have languished in jail, forfeiting eight years of their lives for a huge lie. And the UN and EU? Why, they’re negotiating, even as you read this.
Eight years of negotiations and all we have are these cynical machinations between a lunatic and a bunch of impotent bureaucrats who don’t really care if these nurses ever see daylight again. The bureaucrats know that we know they have no leverage and they don’t care that we know.
Like the Emperor’s clothes, it’s all for show.
The power of the UN continues to appall.
I was not aware. Yet my arm does not need to be twisted to know how simple it would be for bureaucracy to permit, or turn a blind, eye to an epidemic of various infections because of a needle shortage.
Still and all, I believe the vast numbers of aids infection is due to anal intercourse, and the children born to infected mothers. The differnces by culture in the rate of aids infection is due to the popularity of anal sex by region.
To my knowledge, only Kenya has elected to deal with this directly and frankly, without euphemism; and only Kenya has seen drastic reduction in transmission.
Understand that, according to CDC, HIV is transmitted 220 times more efficiently through anal intercourse compared to conventionally. Well, conventional to me. When people in Kenya got the drill, they made it convention also.
But I suppose if it’s acceptable for bureaucrats to spread infection through dirty needles, it’s acceptable to speak in eupemisms about HIV transission.
Xlbrl,
Check out the practice of dry sex in Sub-Saharan Africa too:
Dry sex is a sexual practice of minimizing vaginal secretions by using intravaginal desiccants, by wiping out the vagina, or by other methods before and during sexual intercourse, thus making the woman’s vagina dry and tight. The practice is supposed to generate extra sensation for the man during intercourse but may be painful or uncomfortable for the woman. The practice is common in Sub-Saharan Africa and is of concern as it increases the chances of transmitting sexually transmitted diseases (STDs) including AIDS, due to vaginal tearing.
There have been numerous studies done to show the rise of HIV infections due to dirty needles.
Here is a German one published by the Royal College of Obstetrics and Gynaecologists:
Exposure to Dirty Needles ‘Significant Cause’ of HIV Transmission Among SA Children
Among other things it says:
A previously published study carried out by the Human Sciences Research Council (HSRC) of South Africa revealed an HIV prevalence of 5.6% among 2–14 year olds. An observation from the same survey noted that white children had an HIV prevalence of 11%, while white adults had one of 5.7%, pointing to an important role for non-mother-to-child transmission.[my emphasis]
Dr Brody and colleagues reject the hypothesis that childhood sexual exposure is responsible for such a high incidence of HIV-infection. They comment that sexual experience in this age group is low (less than 2% of under 15 year olds in the South African study) and that despite media coverage of infected men seeking virgin girls as a ‘cure’ for their HIV infection, few cases have been documented.
They suggest a more reasonable hypothesis, supported by other evidence, is that children are infected through non-sterile medical procedures. Dr Brody writes: “Not only are injections popular among African patients, administered at an estimated 90% of medical visits, but also often unnecessary, and injection equipment is often reused without sterilisation.” He concludes that: “The common belief that 90% of HIV transmission in Africa is driven by heterosexual exposure is no longer tenable.” And adds that doctors: “… must educate their patients in the dangers of non-sterile injections and ensure that their own practice is beyond reproach.”
Dirty needles aren’t as sexy a cause of HIV in children as the hypothesis that their mothers are not practicing safe sex, but it more closely explains the statistics of infection.
Note: this is South Africa. Its rates are somewhat lower, but the root cause is the same.
In 1976, the Israelis gave us the copybook solution to the plight of hostages in terror states. Then, it was Entebbe in Uganda. Today it is Libya.
It may take a larger force than Entebbe, and it may be a bloodier action, but a military solution is the only one that will work.
One cannot “negotiate” for eight years. Eight hours, or days, yes. But not years. That is not negotiation.
As to the plight of the hostages of improper or deficient medical care, there is no quick answer. But if the statistics you mention, 20 -40% infected by reusable needles, are correct, then this must be addressed. Immediately.
Heaven knows, it can’t be for the lack of money.
Trackbacked by The Thunder Run – Web Reconnaissance for 07/08/2007
A short recon of what’s out there that might draw your attention updated throughout the day…so check back often. This is a weekend edition so updates are as time and family permits.
exile–
I agree with the Israeli template. However, I don’t see Bulgaria, the UN or the EU applying the Zionist Cure, do you? Those nurses were only there because of the lousy economy of Bulgaria. I presume the same is true of the Palestinian doc.
A Bulgarian MD in the Middle East wrote me after the first post and reported that he does not feel safe, but has nowhere else to practice his profession. I tried to get him to guest post but I think it’s too scary to contemplate being found out and ending up like his countrywomen in Libya.
Here’s some info from 2004:
U.S. Government Awards Retractable Technologies Safety Syringe Contract for Africa under Global HIV/AIDS Initiative
Here’s a snip:
LITTLE ELM, Texas — Retractable Technologies, Inc. announced…that it has been awarded a U.S. government contract to supply VanishPoint(R) safety syringes to five African countries under the Bush Administration’s Global HIV/AIDS initiative (President’s Emergency Plan). Under the contract, which is the first awarded for safety syringes under this program, Retractable will immediately supply VanishPoint(R) syringes to Botswana, Cote D’Ivoire, Ethiopia, Kenya, and Nigeria.
Retractable is the sole U.S. syringe manufacturer to receive a contract under the President’s Emergency Plan, which was launched by President Bush…as a rapid intervention strategy to prevent seven million new HIV infections in fourteen AIDS ravaged countries in Africa and the Caribbean. Countries covered by the program were given the opportunity to evaluate and indicate the syringes they preferred from among all those available worldwide. International health organizations have long recognized that the reuse of syringes in these countries plays a significant part in the HIV pandemic. VanishPoint(R) automated retraction safety devices not only prevent reuse but also virtually eliminate accidental needlestick injuries and minimize hazardous medical waste, a major problem in developing countries.
The Honorable Charity Kaluki Ngilu, M.P., Kenya’s Minister of Health, said: “Kenya recognizes the importance of good syringe technology and is delighted to finally bring VanishPoint state-of-the-art technology to Kenya under the President’s Emergency Plan. The selection of these devices is important to Kenya because they prevent our nurses and other medical personnel from being exposed to dangerous contaminated needles.” She added: “When I first saw the VanishPoint syringe demonstrated at the International Conference on AIDS in Nairobi last September, I knew this technology could become a key part of an effective AIDS prevention strategy. Immediate implementation of these devices through initial funding from the U.S. will have far-reaching effects in the fight against AIDS in Kenya.”
“We are deeply gratified for the opportunity to help protect African patients and healthcare workers from potentially contaminated needles,” said Thomas J. Shaw, President and CEO. “We commend the U.S. administration and Congress for implementing this landmark program, and we are committed to working closely with African and Caribbean health ministries and U.S. agencies and their contractors to immediately supply these devices to help prevent transmission of HIV.” Shaw went on to say that “this contract represents a milestone in the fulfillment of the original mission of our company, which was and is to halt the spread of HIV/AIDS and other bloodborne diseases in Africa by preventing syringe reuse and needlestick injuries. This is a war on AIDS, and our employees and shareholders are proud to be playing a part in it.”
Not too long before this, BDC lost an anti-trust suit for trying to keep RT off the market:
Becton Dickinson and Co Loses
Becton Dickinson & Company, the world’s largest manufacturer of medical syringes and needles, said yesterday that it would pay $100 million to settle a competitor’s accusations that it had illegally manipulated the hospital supply market for years.
The competitor, Retractable Technologies, a need
le maker, had filed an antitrust suit saying it had been largely shut out of the hospital market for its products, which are intended to better protect health care workers from accidental nicks that can transmit blood-
borne diseases.
And here’s another link that disputes the emphasis on sexual transmission of HIV in Africa:
Challenging the Conventional Hypothesis
Dymhpna: In other words, “safe sex” is not the major problem.
This is not the correct conclusion based on the report you refer to. It says:
An expanding body of evidence challenges the conventional hypothesis that sexual transmission is responsible for more than 90% of adult HIV infections in Africa.
…
Taken together, our observations raise the serious possibility that an important portion of HIV transmission in Africa may occur through unsafe injections and other unsterile medical procedures.
…
Though promotion of safe sexual practices remains a priority, new interventions may be required to minimize risk from iatrogenic transmission.
The report suggests that sexual transmission attributes for less than 90%, while pointing out “the possibility that HIV transmission through unsafe medical care may be an important factor in Africa’s HIV epidemic”. Which could mean e.g. sexual transmission 80%, dirty needles 20%.
There are of course many sources, and a complex issue to study. And I doubt it that they have studied the effects of dry sex very closely. It’s just to icky, isn’t it? Nevertheless, the issue about dirty needles should be addressed, since this is an easy one to deal with. But as far as I know (by hearing from people who work down in Africa) this has been addressed all along, and the result is as we can read here.
The report does not suggest that safe sex is not the major problem, and it stresses that “promotion of safe sexual practices remains a priority”. E.g. the practice of dry sex (which I read about the first time in a Danish paper, of course) is incompatible with the use of condoms (which require lubrication to avoid breakage). This is one of the many cultural problems in Africa to deal with regarding this issue.
Conservative Swede–
I have not been clear. “Safe sex” does not correlate with pediatric HIV statistics.
These nurses have been in jail for 8 years because they supposedly transmitted HIV to the hospitalized children when the real story shows that the kids had it before the nurses ever came into the country.
I’m not talking about adult sex, which is the only thing being pushed by the ngo’s and WHO. I’m talking about how to avoid HIV in children and how that relates to the plight of the incarcerated medical staff from the hospital in Benghazi.
Google dirty needles HIV African children and you’ll get both sides of the issue. Some people believe as you do.
In this post, which is about the blame assigned to the Bulgarian nurses for the HIV these children acquired, your thesis about the form of sexual congress the adults engage in is not relevant. Icky, as you say, but OT.
Google video titled INJECTION!.
1 hr 22 min – Sep 25, 2006
THE PRODUCERS OF THE FILM ARE OFFERING INJECTION FOR FREE ON-LINE WITH THE HOPE OF HELPING THE BENGHAZI SIX.
Injection is the real-life story of six health care workers falsely accused and jailed by an Arab dictator, the deplorable conditions that led to their arrest, and the simple solution that might have prevented not only this injustice, but millions of needless infections.
In Libya in 1999, five Bulgarian nurses and a Palestinian doctor were arrested and convicted of infecting over four hundred Libyan children with HIV in a Benghazi hospital. Libyan dictator Moammar Khadaffi proclaimed before the trial that the nurses conspired with the American CIA and the Israeli Mossad to maliciously infect the children.
Widespread reuse of disposable syringes is responsible for as many as seven million cases of AIDS in Africa. Public health officials are reluctant to discuss this problem, perhaps in fear that Africans will avoid critical medical care, such as inoculations for malaria and other virulent diseases. The thrust of public AIDS prevention campaigns is on safe sex, and healthcare risks are critically overlooked.
In this investigative documentary, Mickey Grant travels to Kenya, Bangkok, Sofia, Benghazi, Tripoli, Rome and London in an attempt to discover the truth. He follows the trail of syringes from hospital to garbage dump, and then back into Africa’s health care system.
You’ll hear moving testimony from leaders of the World Health Organization, Amnesty International, African government officials, the Khadaffi opposition, journalists, medical scientists, doctors, and health care workers. You’ll also hear from one of the accused, the son of Moammar Kaddafi, a spokesman for the infected children, and other participants.
Could these healthcare workers have committed this horrific crime? Or, are they scapegoats to divert attention from institutional shortcomings? Is Moammar Khadaffi responsible for this tragedy? Is re-use of contaminated syringes a common practice in Libya and the rest of Africa? Are safer syringes available, and if so, why aren’t they in common use?
For more information, visit http://www.INJECTIONTHEMOVIE.COM
Absolutely, Dymphna. If we confine ourselves to talking about pediatric HIV statistics, this changes the picture in the way you indicated.
I never meant to be OT. I hope people appreciated my comments nevertheless.